POST OPERATIVE REHABILITATION Update v8.2 Jan 2022
Following meniscal transplant surgery rehabilitation is key to recovery.
The University Hospital Coventry & Warwickshire Post- Operative rehabilitation programme is shared below.
After surgery your surgeon will advise you of their specific requirements dependent upon individual surgery and long term goals.
POST OPERATIVE REHABILITATION Update v8.2 Jan 2022
Knee Surgeons: Mr Tim Spalding, Mr Pete Thompson, Mr Andy Metcalfe and Mr Feisal Shah
Outline

Important overview of the procedure and recovery
Meniscal Transplantation involves insertion of a donor Meniscus into the knee to treat symptoms of knee pain that can happen after removal of the meniscus following injury. Treating a torn meniscus (often known as the ‘cartilage’) is a common procedure but not everyone gets problems afterwards, but sometimes pain and limitation in activity may occur and then replacement with allograft donor meniscus is an option.
Meniscus grafts are matched by exact dimensions and are stored frozen. Sometimes it can take a long time to find a suitable graft but once inserted and healed it can function as a ‘nearly new’ shock absorber protecting the joint surfaces and relieving pain and discomfort.
A key part of the operation is the postoperative care and there are many factors to be considered during rehabilitation after meniscal transplant. Early movement and function must be balanced against allowing time for the meniscus to heal in place.
This document aims to guide you through a goal orientated programme to restore good knee function. Loading of the meniscus, through weight bearing and full bending of the knee, must be controlled in the early phases of rehabilitation due to the increased force that is placed on the fixation of the new meniscus.
The meniscus is an important cushion in the knee protecting the joint surfaces and it must heal in the right position before being loaded in activities of sport, running or squatting. Progression through the phases of rehabilitation is based on achievement of criteria and the state of the knee rather than a specific week by week basis. Approximate time points are given as a guide.
PHASE 1: RECOVERY FROM SURGERY
The initial post-operative phase usually lasts the first 6 weeks. The main priorities during this period are to control inflammation and swelling.
PHASE 1: RECOVERY FROM SURGERY GOALS
– Get your knee straight
– Control pain and swelling
– Get quadriceps muscles firing
WEIGHT BEARING
You will be taught how to use elbow crutches before you leave hospital. You should use these to help you to be non-weight bearing for the first 4 weeks after surgery. You must not put any weight through you operated leg until after 4 weeks from your operation as guided by your consultant.
When you are standing at rest e.g. cleaning your teeth, making food/drink you may rest your foot on the floor – however you must still not take any weight through your operated leg.
KNEE BENDING
For the first 6 weeks bending is limited to 90 degrees. Beyond that will compromise healing of the graft.
BRACING
After meniscal transplant surgery you will be fitted with a brace to help limit your range of movement and also provide you with some support.

The brace should be worn day and night for the first two weeks after surgery (it can be removed for washing and dressing).
After this 2 week period the brace can be removed at night to sleep.
At 4 weeks a functional brace will be given to control the force through the knee. It should be worn when walking up to the 3 month point post-operatively.

Partial weight bearing can start at 4 weeks in the new brace with full weight allowed at 6 weeks.
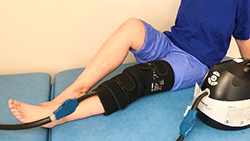
COLD TREATMENT
Cold treatment after your surgery is very important, aiming to keep the swelling of your knee under control, help with pain relief and supports your own body’s natural healing abilities. A cold compression sleeve is usually applied in hospital and you should use an ice pack or cold compression device on your knee for 15-20mins every two hours during the day for the first 7-10 days after your operation.
After 10 days, you can continue to use ice and compression after your exercises if you find it helpful.
ELEVATION
During the first phase of your rehabilitation, you should be resting your operated leg for most of the time. Your leg should be elevated with knee straight and your ankle higher than your hip. This helps to keep the swelling under control in your knee.

NUMBNESS
Patients often describe an area of numbness around the operation site. This is not unusual as the small skin nerves are cut in the operation. Moderate symptoms of numbness and tingling around the knee are common. However, if you are concerned or these symptoms worsen please advise your physiotherapist.
EXERCISES
Exercises are essential but it is important to be careful and avoid damaging the new graft or ‘cushion’ in the knee. Although you are likely to be in some discomfort after your surgery it is vital you complete the exercises below to regain movement and activate muscles after your operation. A physiotherapist will teach you these exercises prior to your discharge home.
- RANGE OF MOVEMENT
KNEE FLEXION
Sit or lie with your leg out in front of you. Place a plastic bag or something to help your foot slide, underneath your heel. Using your hands to support your leg, gently bend your knee by drawing your heel towards you. Repeat 10 times.


Remember not to push flexion beyond 90 degrees for the first 6 weeks.
Don’t be tempted to do exercises that bend the knee whilst your foot is not supported, as this puts high load on the graft.
KNEE EXTENSION
Sit with a small rolled towel under your ankle without anything underneath your knee. Allow gravity to help to passively stretch your knee. Do this for maximum of 2 mins, rest, repeat 3 times.

It is very important to regain full straightening of your knee in the first 6 weeks.
- STRENGHTENING
STATIC QUADRICEPS
Lie on your back with your knee straight. Pull your toes up towards you, push your heel away and tighten the muscles in your thigh. Hold for 10 seconds.
During this exercise, you should feel your patella (kneecap) move upwards towards your hip. Due to the location of your surgery, this may feel uncomfortable but it is important to remember you will not be doing your knee any harm.


STATIC HAMSTRINGS
Sit with your knee slightly bent, push your heel into the bed, tightening the muscles at the back of the leg. Hold for 5 secs. Repeat 10 times.

3. STRETCHING
CALF STRETCHES
Sit with your leg out straight. Loop a strap around your foot; pull the ends of the strap towards you until you feel a stretch at the back of your leg.
Hold for 30 seconds, repeat 3 times .

HAMSTRING STRETCHES
Sitting on a firm surface, with both legs out straight in front of you. Try to ensure both legs are as straight as possible. Lean forwards and reach towards your toes. Hold for 30 seconds. Repeat 3 times.

MUSCLE STIMULATION – optional
After surgery some patients initially struggle to regain good quadriceps control and activation. If this happens you may be issued with a muscle stimulation device. It is advisable to use this as per your physiotherapists’ guidance. It is at the discretion of your consultant and physiotherapist whether you will require this device as part of the rehabilitation program.

CRITERIA FOR PROGRESSION TO PHASE 2:
- Full extension to 0 degrees
- 90 degrees flexion
- Minimal swelling
- Minimal pain
PHASE 2: STRENGTH & NEUROMUSCULAR CONTROL (6 weeks – 6 months)
Regaining muscle strength, balance and core strength are the goals of phase 2 – BUT WITHOUT OVERLOADING THE GRAFT.
In order to progress through this stage, the knee must be ‘quiet’ – not swollen and inflamed. Increases in pain and/or swelling indicate that the knee is not yet able to tolerate an increase in load of exercise.
PHASE 2: STRENGTH & NEUROMUSCULAR GOALS
– Achieve good single leg balance
– Regain good muscle strength
– Restore ‘normal’ gait
This phase is essentially CYCLING and WALKING.Squatting is NOT ALLOWED as this puts load on the graft and surfaces.No running or other high impact activities are permitted at this stage of rehabilitation.
1. CYCLING
Cycling on a static exercise bike is the most favourable exercise to do at this stage. Given the nature of the surgery you have had, cycling provides the least impact whilst still working the musculature around your knee appropriately. We advise to start on the bike positioned with the seat as high as is comfortable and with no resistance applied. Once you can complete 20 minutes of cycling at this level then slowly increase the resistance with each subsequent session.

2. WALKING
Walking is also a recommended exercise, on land or in a swimming pool. Monitor the response of your knee regarding swelling and pain to gauge the appropriate time and distance to walk. If your knee does not swell or become painful then you are able to gently increase the time and distance. We do not recommend breaststroke at this stage.
3. Lower Limb Strengthening
Quadriceps(as per phase 1)
Static quads and Inner Range Quads (IRQ) with low load. Should be able to feel the load in quadriceps thigh muscles.
Calf Raises
Stand on the edge of a safe step. Engage your core. Make sure the balls of your feet are solidly planted on the edge of the step with your heels over the edge. For safety, begin this exercise with a wall or railing nearby to hold on to for support. Keeping your legs straight lift your heels up, hold for three seconds and gently lower heels until they are below the step level. Complete 12 times.

Hip Abduction
Lying supine, with a plastic sheet/bag under the operated leg. Tighten your abdominals and glute muscles. Slowly slide the leg out to the side, ensure not to lift the leg as this will activate a different muscle group. Complete 12 reps, repeat 3 times.
Hip Adduction
Lying with your knees bent, place a pillow between your knees and gently squeeze. Hold the squeeze for 5 seconds. Repeat 10 times. Gently increase repetitions as your pain allows.
Hip Extension
Standing supported by a chair or work surface, tighten your abdominal muscles. Raise one leg backwards, keeping your knee straight until your foot is approximately 3 inches off the floor. Hold for 3 seconds, then slowly lower. Ensure you do not lean forward, remain standing tall. Complete 12 reps, repeat 3 times.
4. Core Strengthening
Pelvic tilts
Lying on your back with your knees bent. Flatten your back against the floor by tightening your abdominal muscles and tilting your pelvis upwards slightly. Hold for 10 seconds, repeat 6 times.
Clam
Lying on your side, arm outstretched in line with your trunk. Allow your head to rest on your arm. Hips bent up to approximately 45 degrees and knees bent up to approximately 90 degrees. Raise the top knee upwards keeping the feet together. Then continue to lower the top leg onto the lower limb.
Plank
In the push up position on the floor, bend your arms to 90 degrees and rest your weight on your forearms. Your elbows should be directly beneath your shoulders and your body should form a straight line from your head to your feet. Aim to hold for 30 seconds with 15 seconds rest, repeat 3 times.
You may also wish to add ‘side plank’ into this exercise for increased core strength.
Supermans(FROM 3 MONTHS ONWARD)
Start on all fours, place a pillow under the knees if required. Ensure your core is engaged and your back is straight. While keeping one arm and knee on the floor extend the opposite leg and arm to fully straighten them. Slowly return to the starting position and repeat the action 5 times on each side.
5.Proprioception
Single leg stance
SINGLE LEG STANCE
Remove shoes and socks. Stand still on one leg for 20 seconds without allowing your elevated foot to touch the ground – vary this exercise with eyes open and closed and arms at your sides or raised. You may need to hold on to the wall or a chair to start with. Repeat 3 x 20 secs daily.

Double leg mini-squats on an unstable surface
Standing on a BOSU or a balance board with both feet, gain your balance. Try to spread your weight evenly between the balls of your feet and your heels. Maintaining your balance and trying to keep the surface of the BOSU/board level. Gently lower yourself into a mini-squat (approx. 30-40 degrees knee flexion).

6. Stretching
CALF AND HAMSTRINGS STRETCHES: As per phase 1 above.
HIP FLEXOR STRETCH
Start in standing. Place your good leg on a chair/bed and your operated leg behind on the floor, which is the one you are about to stretch. Keeping the hips pointing forward, back straight, squeeze your buttock muscles and bring your hips forward to feel a stretch around your groin.
Hold for 30 seconds and return to starting position. Repeat 3 times on both legs.
CRITERIA FOR PROGRESSION TO PHASE 3:
- At least 120 degrees flexion
- No pain
- Minimal swelling
- 80% quadriceps strength of non-operated side
- Y-balance test
- Y-balance test: < 4cm difference in anterior direction to non-operated side
PHASE 3: END STAGE REHABILITATION AND RETURN TO APPROPRIATE ACTIVITY (starting 6 months following surgery)
PHASE 3:REHAB AND RETURN TO APPROPRIATE ACTIVITY
– Adequate strength, power, neuromuscular control, symmetry and stability for
patients’ specific goals
– Functional Movement Training
– Safe, guarded return to low impact sport
Contact sports should be avoided until at least 12 months and only after careful discussion.
Continued Strengthening
All major muscle groups of the core and lower limb will need to be strengthened further. Large deficits in individual muscle groups can have a significant effect on functional ability and your eventual return to function. Effectively you are only as good as the weakest link in the chain. Our aim is that each patient should be assessed individually to identify the specific areas of weakness needing to be addressed.
There also needs to be a balance of the types of exercises undertaken.
Exercises such as squats and lunges work the muscles hard, but they also put a high degree of force through the joint and meniscus, which is not advisable e.g. deep squatting >90degrees, high weight leg press. There needs to be a balance of continued endurance and strength training.
Functional Movement Retraining
Good movement patterns will need to be retrained and practiced to help maximise the life of the new meniscus as well as ability to return to functional goals. This is all about trying to make the muscles work well together as a team. Muscles are your shock absorbers.
Poorly controlled and co‐ordinated movements when stood still, and then when moving, will potentially put excessive load through the knee and meniscus. Return to sport and function will then have a higher risk of failure, e.g. when bending on one leg your knee should stay in line with your second toe, and your pelvis level and straight. This pattern will be perpetuated through functional return unless trained otherwise. This is similar to the skills training done in all sports to maximise ability.
This stage takes time and practice: it is about quality of movement, not number of repetitions. Some movement patterns may have been present for a long time and will feel automatic and normal, although they are not ideal, and should be trained out with focussed work.
Low load safe guarded return to sport
Aim for progression through increasing level of skills and drills as strength and movement patterns progress. It is imperative this is patient specific and depends on goals for return to activity. This is the vital last piece of the jigsaw. If muscles of the lower limb are not used in a safe co-ordinated way then the hard work of rehabilitation to this point will not be best put in to practice.
The table below illustrates the characteristics of sports we feel should be avoided following meniscal transplant.
Discussions should be had at twelve months following transplant surgery to finalise end stage goals. These goals will be dependent on many factors including state of the meniscus and joint surfaces of the knee at this stage.
| High Risk Sports
and factors |
Lower Risk Sports |
| Repetitive impact with cutting and pivoting | Aerobic low impact sports |
| Contact sport | Moderate sports participation |
| Competitive situation | Non-contact sports |
| Playing position on field | Cycling |
Contributing Authors
Knee Surgeons
Tim Spalding
Andy Metcalfe
Pete Thompson
Feisal Shah
Specialist Physios
Laura Asplin
Nicole Bausch
David Wright
Kelly Hollway
Ivor Hughes
A MESSAGE FROM YOUR CONSULTANT
Meniscal Transplant surgery has been performed for over 25 years worldwide and in Coventry since 2002.
It is an exciting option to improve symptoms in the knee due to lack of the cushioning effect of the Meniscus. As a donor graft tissue is from someone else it cannot be considered normal and we remind you that the aim is to buy time for the knee – improving your function and enjoyable activity level, and maybe preserving the joint.
You are clearly part of the process. As surgeons we have half the job and the other half is down to you and the physio, hence the detail in this rehab guide.
Remember that it used to hurt when squatting and jumping on the knee? – these activities hurt because that is where the meniscus was unable to protect the joint and came under load. These activities need to be avoided until the right time as indicated in the guide.
It takes a year or so for the knee to fully mature after this surgery and your help is needed in buying into this concept of preserving your knee. We have had many successes, but we still have a few less successful results.
To help us improve our treatment we need data, and we ask that you will be part of our Surgery Outcome Program, responding to our questionnaires documenting your progress. This helps us optimise treatment for you and others.
We wish you all the best in your recovery and hope you can be like our happy patient Bryony!

A Message to your Physiotherapist please
Thank you for taking on the care of our meniscal transplant patient. Following our experience and the growing international knowledge of this surgery we have provided this document to help guide your rehabilitation strategy.
Meniscal transplant surgery is the implantation of a donor meniscus to the patient via arthroscopic surgery. The meniscus is held with fixation sutures through bone tunnels, hence very different surgery to a meniscus repair, where early weight bearing is allowed.
As per the guidelines above the protection of the new meniscus is paramount in the post-operative rehabilitation. Biomechanical research shows how forces on the meniscus change through ranges of flexion. As the knee flexes beyond 30 degrees, increased force is placed on the posterior horn of the meniscus. At 90 degrees flexion, the stress on the peripheral meniscal repair site is 4 times higher than in full extension. Further deep flexion of the knee to a full squat position, causes large translations of the femoral condyles and increased compressive stress on the meniscus and the joint surfaces is designed to protect. Most patients already have some damage on the important joint surfaces.
Due to these findings there must be no squatting/ lunge/ split lunge activities for at least 6 months post operatively to limit the compressive stresses on the new allograft.
Open kinetic chain exercises, even without additional resistance has been shown to produce tibio-femoral shear forces in the range of 500N which exceeds the strength of the initial meniscal fixation.
Cycling and walking put the lowest shear force and compression on the meniscus and joint surfaces.
These principles are the main basis of the protocol for the first 6 months after surgery. The meniscus has to bed into the correct position in order to support the joint, hence no impact exercise is advisable until after 6 months.
If you have any questions regarding the rehabilitation of your meniscal transplant patient please do not hesitate to contact our team at University Hospital Coventry & Warwickshire on 02476 965098.